
Get the most reliable climate data
Oops! Something went wrong while submitting the form.
.webp)


What this blog covers
ends with a simple thought: Maybe the problem isn’t effort. Maybe it’s timing.
{{key-insights}}
The allergy prescription market lives and dies in a 10-14-day window. Not during peak pollen season or the biggest marketing push, but right when symptoms start.
Most pharmaceutical companies miss it entirely. Their outreach to doctors begins weeks after patients have already chosen a treatment.
Here's the problem: Most companies plan their allergy campaigns using last year's pollen data. But allergy seasons no longer follow last year's patterns.
So, if you are responsible for HCP engagement at an Allergy Rx brand, here are seven structural reasons plans quietly break down before competition takes your prescription share.

Almost all allergy brands plan their HCP engagement cycles around historical "peak weeks," which are technically the reliable spring windows when pollen typically surges, and patients flood into clinics.
But this timeline stopped being reliable a while back.
Analytics & forecasting tools started capturing patterns, which, again, made things static.
The problem is, that calendar stopped being reliable a while ago. Weather patterns shifted, exposure started earlier or later depending on the city, and symptoms no longer followed a neat national curve. Some regions now see multiple smaller waves instead of one clear peak. Others experience early exposure with delayed patient action.
What looks stable in historical averages breaks down on the ground. And yet, most engagement plans are still anchored to the same old weeks, assuming patient behavior will catch up. Increasingly, it doesn’t.
Research shows pollen seasons across North America have lengthened by ~20 days, and pollen concentrations have risen by ~21%, largely driven by climate warming. Tree and grass pollen do not wait for brand calendars or budget unlocks.
Where HCP engagement plans fail:
So when a campaign launches based on last year's calendar, the real surge has often already happened. Patients have made appointments, doctors have written prescriptions, and the critical prescribing window has closed before the first sales call, or email even reaches a physician's inbox.
By the time marketing budgets unlock, and your HCP engagement plan is activated, the season's already moved on without you.

All allergy therapies do not behave the same once symptoms begin, and that difference quietly dictates how demand actually forms in the market.
Decongestants like Sudafed and topical sprays such as Afrin can deliver noticeable relief in under 30 minutes. Oral antihistamines, including Claritin and Zyrtec, typically start working within a few hours and can prevent symptoms when taken consistently. Nasal steroid sprays, such as fluticasone-based therapies, often require upto 2 weeks before they reach full clinical effectiveness (source: GoodRx.com).
From a clinical standpoint, this is well understood. From a commercial planning standpoint, it is often underweighted.
That difference in onset time creates a narrow but critical requirement for HCP engagement. Therapies built for prevention only work commercially if physicians and patients are aligned before pollen exposure rises.
Most engagement plans still ramp up around peak symptom weeks. By then, patients are already uncomfortable, and physicians are under pressure to deliver immediate relief. The conversation shifts from prevention to speed.
If doctors and patients weren’t primed earlier, daily therapies lose relevance. Brands stop shaping behavior and start competing on immediacy, a battle they are unlikely to win.
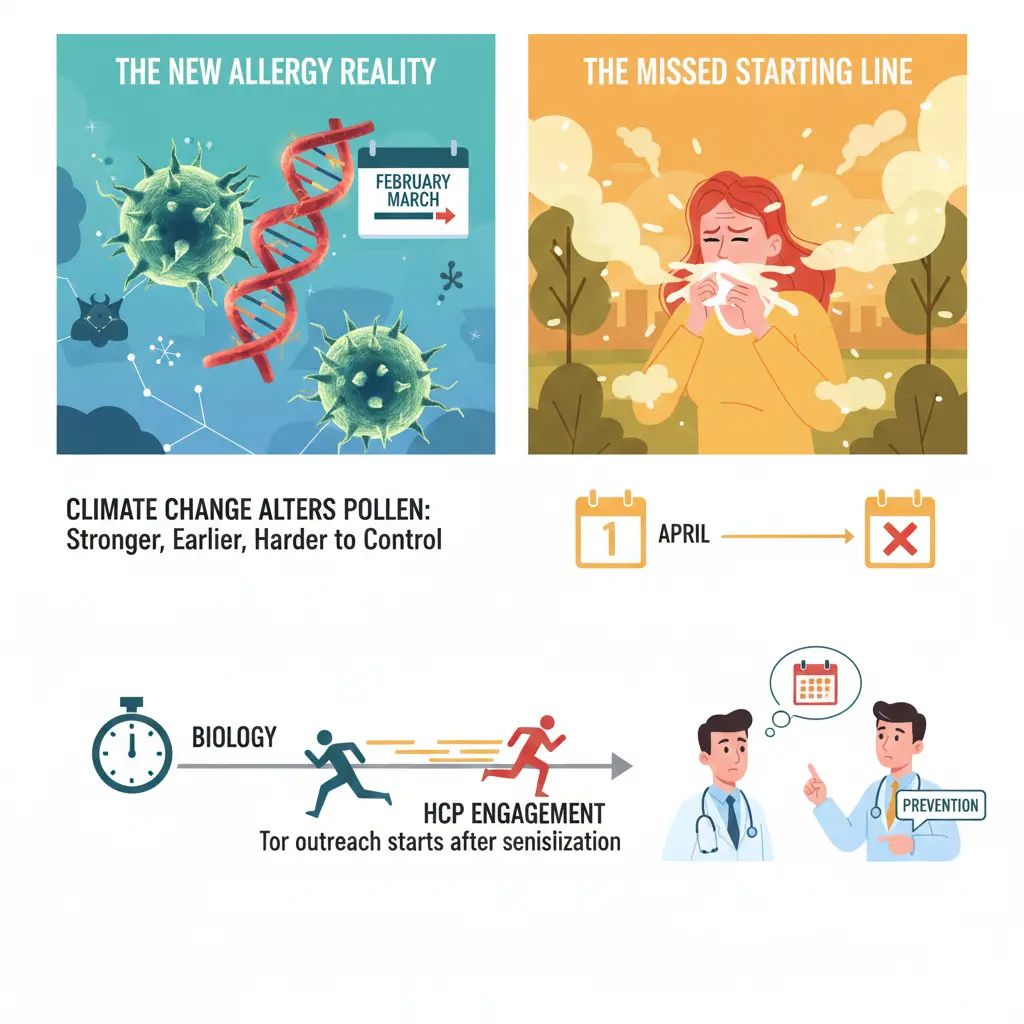
Stretching allergy seasons by a few weeks was last year's problem. Climate change has started to fundamentally alter the biochemistry of pollen itself.
In the study, Pollen respiratory allergy: Is it really seasonal? Published by the World Allergy Organization, they cited evidence for the same.
Pollens that cause allergic reactions originate mainly from grasses, weeds, and trees. Pollen grains (2.5–10 μm), male reproductive structures of plants, are a major causal agent of respiratory allergy (source: Immunology and Allergy Clinics of North America - Science Direct, Study 1, Study 2).
These plant-derived pauci-micronic components include stem particles, trichome parts, plant debris, and carry allergens which can produce allergic symptoms (source: Immunology and Allergy Clinics of North America - Science Direct, Study 2).
They enter the human body via the upper respiratory tract mucosa and cause allergic sensitization. As a result, symptoms are becoming stronger, earlier, and harder to control with standard approaches.
Where plans fail:
What this changes, commercially, is the starting line.
When pollen becomes more potent and sensitization begins earlier, the first patient visit is no longer the first point of exposure. By the time symptoms surface, the immune response is already underway. HCP engagement that still starts at symptom onset is already behind.
Your outreach plans fail not because the science is misunderstood, but because engagement begins after the biology has already done its work.

That predictability has steadily eroded. A warm February can trigger early pollen release in parts of the southern United States, while northern regions remain frozen for weeks.
Most allergy engagement plans still assume a national season and historical curves, driven by a single start date and a shared set of peak weeks. In reality, allergy exposure unfolds region by region, shaped by local weather, vegetation, and urban conditions.
Warmer, earlier springs have materially extended pollen exposure windows across the U.S. An analysis of temperature trends in 198 U.S. cities found that 87% experienced longer freeze-free growing seasons since 1970, with an average increase of 20 additional days, and some cities gained three or more extra weeks. The result is earlier pollen release, longer seasons, and wider regional variation that no national allergy calendar can accurately capture (source: Climate Central).
"There are these extreme, chaotic conditions that climate change is associated with," explains Kari Nadeau, chair of Harvard's Department of Environmental Health. "And that warming is affecting our pollen seasons."
Where plans fail:
When HCP engagement, media, and field activity are synchronized nationally, they inevitably arrive too early in some markets and too late in others. The result is wasted effort where risk is low and missed opportunity where sensitization has already begun.
The same email blast, the same messaging, the same timing sent to allergists in Atlanta and Minneapolis alike. So a doctor in Georgia receives campaign materials in March when their patients started showing up a month earlier, while a physician in the upper Midwest gets pitched on spring allergies weeks before anyone in their practice has symptoms.
Despite these shifts, much of pharmaceutical outreach remains anchored to outdated national schedules. The same email campaigns, messaging, and timing are still sent to allergists in Atlanta and Minneapolis alike.
To a physician already seeing allergy patients, the brand feels late.
To a physician not yet seeing symptoms, the brand feels irrelevant.
Either way, credibility takes a hit.
Let’s understand with an example.
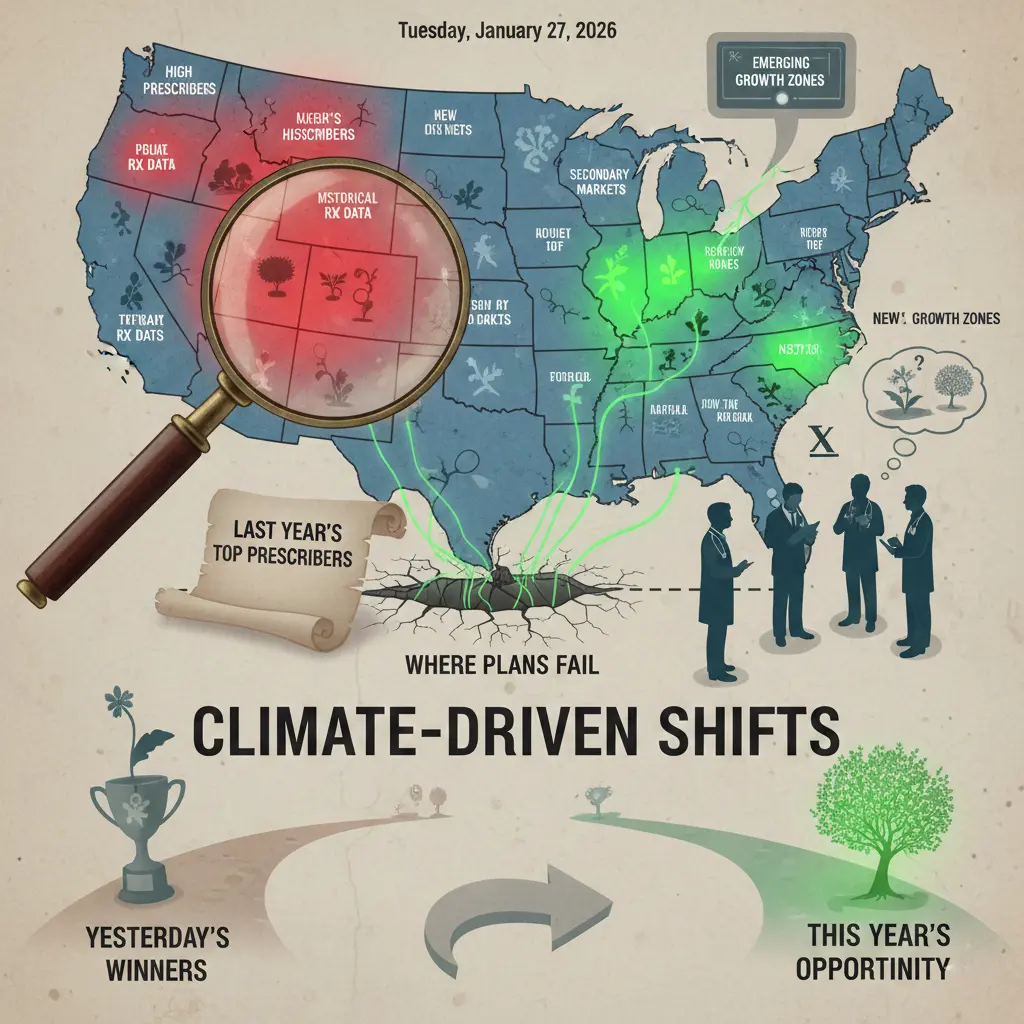
Imagine planning emergency response resources for hurricane season by looking at where last year's storms hit. You'd staff up Miami because that's where the damage was, even though this year's systems are tracking toward the Carolinas.
That's essentially what's happening with pharmaceutical targeting strategies right now. Most companies are still building their allergy campaigns around historical Rx sales data or limited climate & pollen trends, not customized to their brand(s).
Where plans fail:
A cross-sectional study found no statistically significant association between cost awareness and brand-specific prescribing preference, suggesting that factors beyond price drive brand loyalty.
When pharmaceutical representatives detail branded respiratory drugs, physicians increase branded prescriptions without reducing overall respiratory drug volume, resulting in purely competitive gain. The elasticity applies to branded market share, not disease class demand.
Why does this matter? Because relying on information such as: which doctors wrote the most scripts, which regions had the highest patient volume, and where to deploy sales reps and marketing dollars.
It's a logical approach when patterns hold steady year over year, and for a long time, they did.
But climate-driven changes are reshaping where the burden shows up.
The result is that new pockets of high patient volume are emerging in areas that pharmaceutical companies have historically treated as secondary markets. And by focusing exclusively on last year's top prescribers, brands miss these emerging zones entirely.
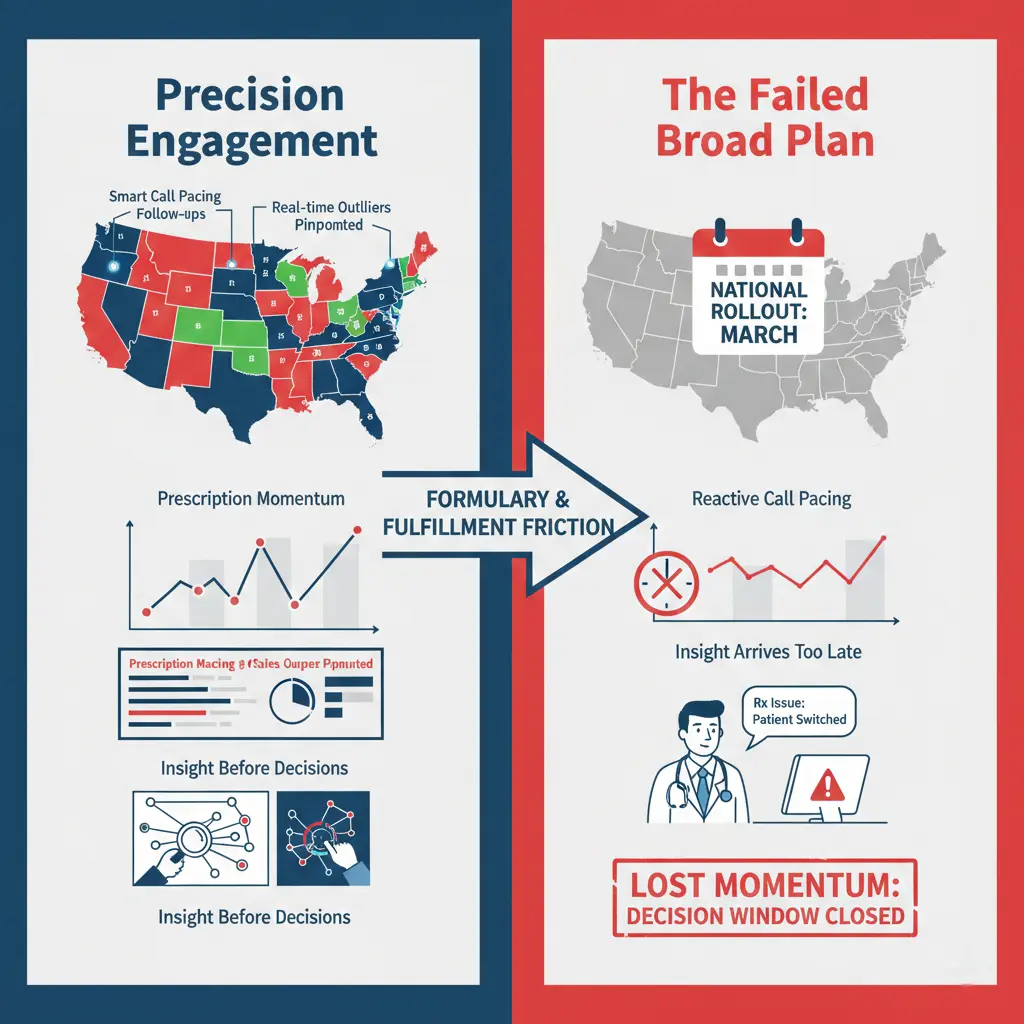
In Allergy Rx, engagement effectiveness is rarely about volume. It is about precision.
The programs that work are the ones meticulously crafted to enhance call pacing, pinpoint sales outliers, and recommend follow-up actions based on real HCP interactions, not static calendars.
When teams understand which physicians are responding, where prescriptions are sticking, and where early friction is showing up, they can adjust field effort and messaging before momentum is lost.
Where the HCP engagement plan fails:
Most plans still activate too late and too broadly.
Call pacing accelerates nationally instead of regionally. Sales outliers are identified only after the spike has passed. Follow-up actions are reactive, not timely.
By the time access or fulfillment issues surface in the data, first prescriptions have already bounced and physician confidence has already shifted. Engagement fails not because teams lack effort, but because insight arrives after the decision window has closed.
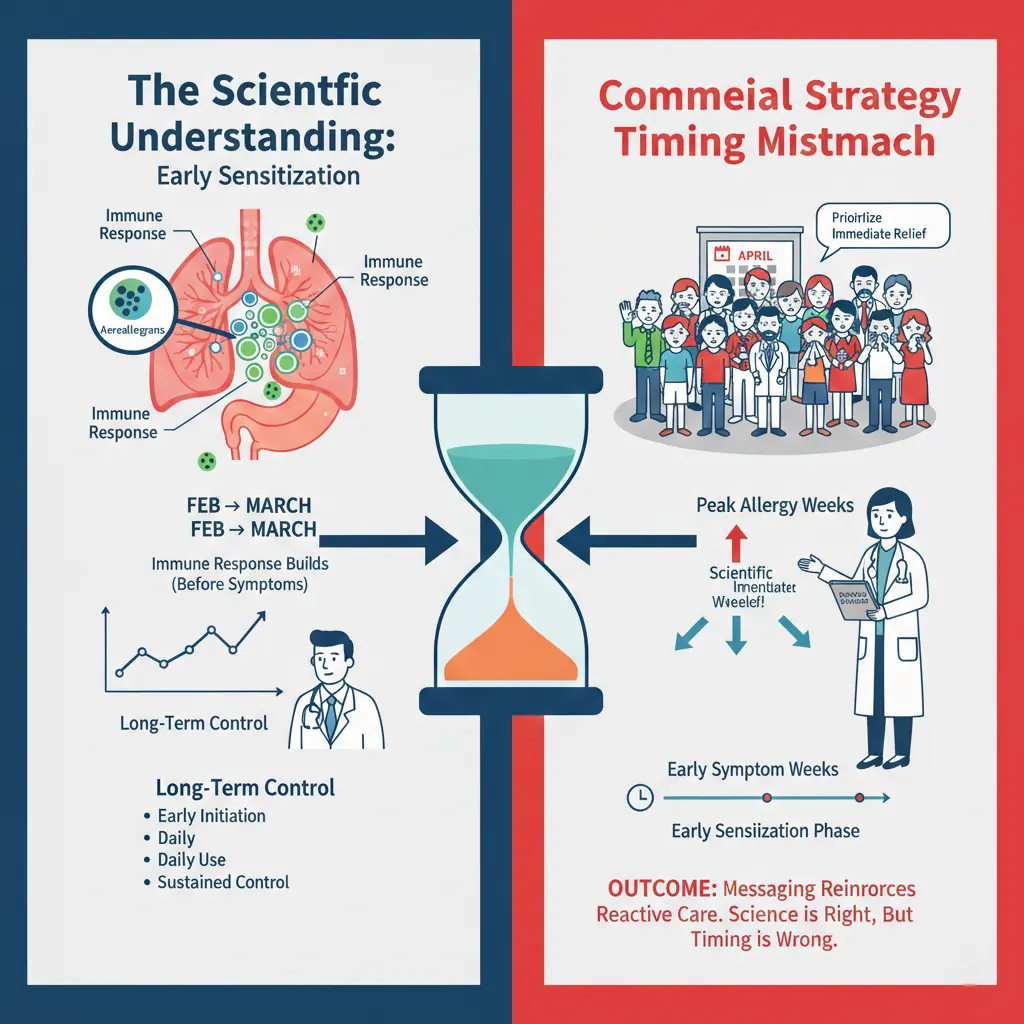
Allergy science has evolved faster than allergy commercialization. Clinically, we now understand sensitization begins with exposure, often days or weeks earlier, as pollen and aeroallergens trigger an immune response that builds before patients seek care. By the time sneezing, congestion, or sleep disruption sends someone to a clinic, the immune response is already well underway.
HCP engagement in allergy still arrives too late. Scientific education around early initiation, daily use, and sustained control is concentrated during peak pollen weeks, when clinics are already managing acute symptoms. In that setting, prescribing decisions prioritize immediate relief, not long-term control.
Engagement is timed to symptoms, not exposure. Field calls, medical education, and follow-ups cluster around peak allergy weeks instead of the early sensitization phase.
As a result, scientific messaging reinforces reactive treatment rather than shaping preventive prescribing. The science is right, but in allergy, timing determines whether it actually changes behavior.
You cannot lead with long-term maintenance when the waiting room is full of patients in distress.
For an allergy brand sales and marketing lead, the most expensive mistake isn’t weak creative or limited reach, as many would assume.
It’s a perfect message delivered at the wrong moment.
While many Rx brands still compete for share of voice, the winners in allergy are competing for share of timing. They synchronize field force activity, market access readiness, and omnichannel engagement with the exact moment climate-driven pollen spikes turn a calm clinic into a crisis center.
In allergy, it's about showing up when it counts.
In the allergy prescription category, the effective engagement window typically spans about twelve weeks. That window is becoming increasingly uneven, shifting by region and changing from year to year.
Platforms such as ClimaChain are designed to address this gap by aligning physician engagement with real-world pollen exposure and symptom emergence as they occur. Rather than anchoring outreach to a predetermined spring launch, engagement is timed to local conditions, which can differ by hundreds of miles and, in some cases, by several weeks.
The result is that clinical messaging reaches physicians during periods when allergy cases are actively presenting and when treatment decisions are being made.








